Know the Differences | Kyphosis, Lordosis, & Scoliosis


The backbone is responsible for so much of our overall posture, and any damage to it can affect how well we function and move, which is why seating for spinal conditions is so important.
When you see a healthy spine from the side, it has natural curves that help to absorb shock and cope with gravity’s effect on the body. When you look from behind, the spine should be straight down the middle of the back.
However, some people have spinal deformities. Whether it’s genetic, a result of poor positioning, illness, or an accident, the spine can curve and become misaligned therefore leading to further health problems.
Scoliosis, Lordosis, and Kyphosis are three kinds of spinal deformities. These are particularly prominent when we examine a person’s seated posture. Knowing the difference between these three irregularities is vital for physiotherapists, occupational therapists, and seating specialists.
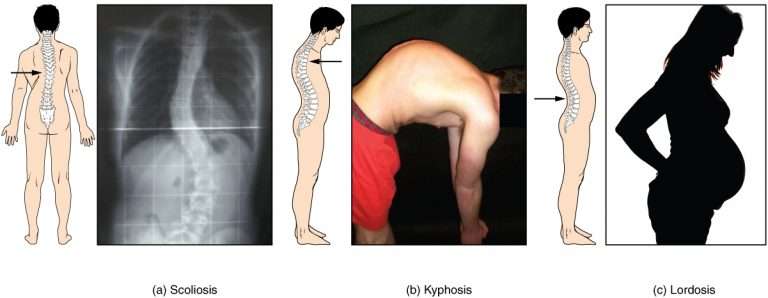
Here you can see the differences between these three spinal conditions.
Kyphosis
Kyphosis relates to the upper part of the back. If you have a particularly rounded upper back (generally with a curvature of over 50 degrees), or your head seems further forward than the rest of your body, then you may have a kyphotic spine.
This can cause damage to physiological function and puts you at risk of developing pressure injuries at the top of the back.
People with a kyphosis sometimes develop pressure ulcers on the back of their heels, as they put an inordinate amount of pressure there to anchor their position. They may also find that their back and legs get tired easily.
This spinal deformity can be caused by posterior tilt in the pelvis or something as serious as abnormal vertebrae or Spina Bifida. Osteoporosis is one of the most common causes of a kyphosis, as vertebrae are more susceptible to decay and cannot support the user’s weight as comfortably.
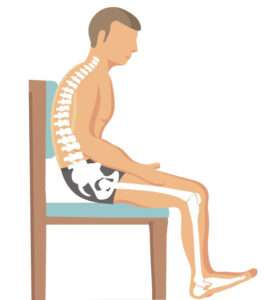
Kyphotic spine
Lordosis
On the contrary to kyphosis, lordosis affects the lower back. This is where you have an irregular inward lumbar curve, meaning that the individual appears to be leaning back a bit.
Your buttocks may also be more pronounced when sat down, or you may have an unusually large arch in your lower back when laid on a hard surface. This can cause pain in the lumbar area that can be relieved with anti-inflammatory medication, or by wearing a back brace.
Building up muscle strength in the abdominals can also help to treat a lordosis. Things as simple as losing weight can also help to relieve the effects of a lordosis.
Having such a severe curve in the lower back can be indicative of an over-rotated pelvis, increased tone in hip flexors, or even having weak abdominal muscles in comparison to extensors. These things can encourage the person’s lumbar to curve forwards too much and create a lordosis. People with achondroplasia may also find that their spine has a lordosis because of their small stature.
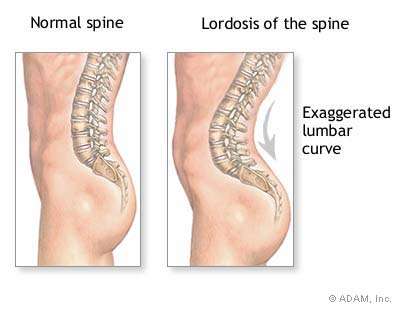
Here you can see how lordosis extends the lumbar curve and tilts the pelvis forwards.
Scoliosis
Arguably the most well-known spinal deformity is a scoliosis. When you look from behind, a scoliosis bends the spine away from the mid-line of the back so that it may become ‘C’ or ‘S’ shaped.
In turn, this may make you stand or sit unevenly, with one shoulder lower than the other. It is clearer to identify a scoliosis when looking from behind as there could be twists in your posture or a shoulder blade or hip that is sitting lower than the other.
The causes of scoliosis are not as clear as lordosis or kyphosis, but it is suspected to be a genetic defect.
Scoliosis is most often associated with pelvic obliquity (a horizontally tilted pelvis), osteoporosis (decay of the vertebrae), or pelvic rotation (wind-sweeping). More extreme scoliosis can lead to compression of the person’s ribcage and internal organs, so it is important for doctors to monitor the curve.
A back brace might be needed for younger people with a scoliosis, but surgery is sometimes needed to correct the spine.
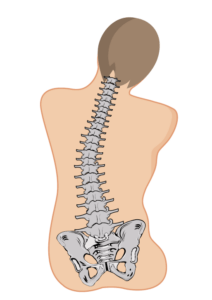
Scoliotic spine
Summary
These three different spinal curves all differ and can cause stresses and pressure on various parts of the body. It’s important to monitor the curve and take action to prevent further damage sooner rather than later.
These spinal deformities will be common terms for physios, OTs and other healthcare professionals, but it’s always good to have a guide handy should you need it. For more information on specialist seating for people with scoliosis, lordosis and kyphosis, download our free Healthcare Professional’s Complete Guide to Specialist Seating Assessments eBook.
Download Our Free Seating Ebook
Our specialists will help you find the perfect solution
FAQs
What is the difference between kyphosis, lordosis, and scoliosis? Kyphosis affects the upper back and causes a rounded spine, lordosis impacts the lower back and results in an excessive inward curve, and scoliosis is a sideways curvature of the spine that can create an ‘S’ or ‘C’ shape.
How do kyphosis, lordosis, and scoliosis affect posture? Each condition affects posture differently: kyphosis causes a hunched back, lordosis exaggerates the lower back curve, and scoliosis leads to uneven shoulders or hips due to sideways spinal curvature.
Is lumbar lordosis normal? Yes, a certain degree of lumbar lordosis (the inward curve of the lower spine) is normal and necessary for spinal balance. However, excessive lumbar lordosis can lead to discomfort and postural issues.
Can you have kyphosis, lordosis, and scoliosis at the same time? Yes, it is possible for an individual to have a combination of these spinal conditions, especially in cases of severe spinal misalignment or structural abnormalities.
How are scoliosis, kyphosis, and lordosis treated? Treatment depends on the severity and underlying causes. Mild cases may require physical therapy and posture correction, while severe cases might necessitate bracing or surgical intervention.
Kyphosis vs Lordosis: What is the key difference? Kyphosis causes an excessive outward curvature of the upper back, leading to a rounded or hunched appearance. Lordosis, on the other hand, results in an exaggerated inward curve of the lower back, making the lower spine appear more arched.
What are the common causes of spinal curvature disorders? Genetics, poor posture, osteoporosis, neuromuscular conditions, and congenital defects can all contribute to spinal curvature disorders like kyphosis, lordosis, and scoliosis.



